On any given day, at any given moment, blood flows through bodies, flesh and viscera, shaping our world from the inside out. The process is rather simple, I have been told: in the human body, blood is propelled by the heart, repetitively flowing from the right atrium and right ventricle, through the pulmonary system, into the left atrium, left ventricle, and aorta. It then unfurls into the rest of the body and back to our starting point, the right heart.
But, blood has never been a single, unified fluid. Among blood’s several components—red blood cells, plasma, platelets—not all have the same exact velocity. Plasma and red blood cells in particular may travel across vascular plains at variable speeds, propelling antigens and antibodies into elusive journeys. And, across different bodies, red blood cells can take various shapes, a trait that characterizes sickle cell disease, one of the most common genetic blood conditions in the world. As a novice, interdisciplinary student of transfusion science & medicine, blood and its innumerable intricacies run not only through my veins, but my thoughts, forming colourful images in grey matter.
But these reflections are more than an intellectual exercise. In the home I grew up in, with a sibling who has sickle cell disease and a mother who dedicated her life and career to paving a better healthcare system for people like him, understanding how blood is analyzed, stored, managed and cared for was linked to broader experiences of harm, stress and pain.
When I began developing my dissertation project, which seeks to ethnographically follow blood across myriad institutions, locales and historical periods, I started to observe different models that helped me visualize blood circulation. On the one hand, I was interested in finding texts, images and charts that could reconfigure the complexities of physiological processes that I had limited technical understanding of. At the same time, I searched for these models because I wanted to see what was lost in them, the stories and vulnerabilities that these facsimiles could not fully replicate.
For me, the question is thus not only how does blood work, but also how is it seen? And how can we better see it?
Model 1
These were among the many, many questions at the heart of the development of the Reference Man (initially called Standard Man), a human physiological model adapted by scientists from the US, UK and Canada in 1949, and later further designed by the International Commission on Radiological Protection.[i] I first came across this model in a context that will be very familiar to fellow graduate students: a seminar where I was introduced to geographer Shannon Cram’s (2023) watershed Unmaking The Bomb.
The aim of the model was to simulate the prototypical body, imagined to be a “typical Western adult male,” that was vulnerable to our increasingly radioactive atmosphere, and measure the various hazards that this body may be exposed to over time.[ii] As is often the case with models, not everything was chosen to be accounted for. Such omissions come into clear view when looking at a 1996 report by US scientists working to specifically update and refine the blood circulation of Reference Man. As they write, the “model is a compromise between physical reality and computational simplicity.”[iii]
Cram brilliantly argues that such models are a product of the Cold War and its ongoing aftermaths, where managing and containing the nuclear industrial complex has emerged as a vital and, also, impossible project. Cram places the Reference Man among a cohort of quantitative simulacra that turn meaningful lives into statistical people. Into a “very specific no one” that generalizes the specificities with which radioactive particles can travel within and without, eroding lives and landscapes.[iv]
Quite similarly, in the 1990s Reference Man blood circulation model, blood flows through arrows into narrow categories, data, papers, reports and ultimately bureaucratic structures in a systematic fashion. As a thought experiment, I digitally reproduced and colour coded the model, seeking to teach myself some of the fundamentals of circulatory fluidity.[v] With each line, rectangle and letter that I retraced, a tangled web of shadow arrows emerged.
In these shadows, I see the messy motions that even computational simulations of blood cannot really hide, even if the directionality of these lines are the product of glitches rather than ‘physical reality.’ Staring into the pixelated flesh, I cannot help but type words that are not entirely my own. I do this to articulate the dissonance of a model that, although accurately portraying the pathways of oxygenated and deoxygenated blood, I am not sure who it represents: “I am not what I am. I am Reference Man” (see Figure 1).
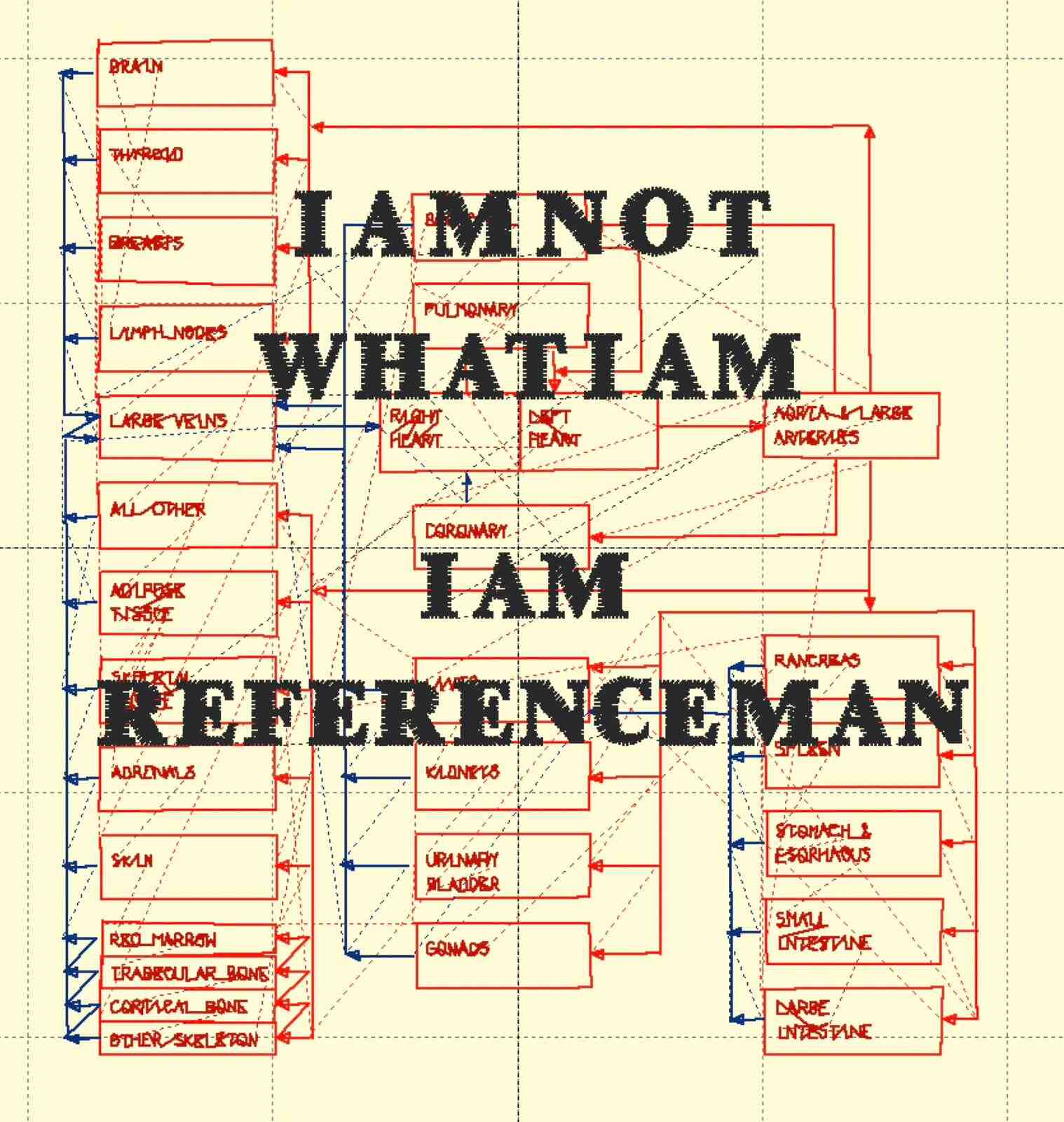
Figure 1. Digitally retraced and colour coded 1996 Reference Man Blood Circulation Model with brief musings from the author. “I am not what I am” is originally from Shakespeare’s Othello, a play that I have long found helpful in thinking about the distorted worlds and representations that can be made in the visage and vision of power. Reworked model by author.
Model 2
I came to know this second model while conducting background reading and research for a report that I am authoring in collaboration with a Canadian sickle cell advocacy organization. The goal of the report is to chronicle emerging efforts by healthcare providers to collect data on the chronic condition, and to develop a national registry that can trace the state of sickle cell care across the country. Though I was initially broadly surveying literature on structural health inequities, one model—John Henryism—stood out as offering a particularly evocative picture of the imbrications across health, history, geography, economy & folklore. From these overlaps, we may see how livelihoods, bodies and blood flows are kept precarious.
Epidemiologist Sherman A. James developed the John Henryism hypothesis & scale during the 1980s-90s through several studies that established a correlation between socioeconomic status and high blood pressure for Black people.[vi] The focus on blood pressure must be situated in the context of the hypertension epidemic that captured the attention of clinicians, statisticians, researchers and the US public in the late twentieth century.[vii] The model, emanating from both a famous folktale and a first-person oral historical narrative that James collected, highlighted that this epidemic of overworked arteries and hearts could only really be understood through the labour histories and mythologies that are constitutive of American life.
To delve into the origins of John Henryism, we will have to shift gears, moving to another historical period: the aftermath of the US Civil War. At this time, the folktale of John Henry, the steel-driving man, emerges. In folklore, John Henry was a Black American man who worked in the Big Bend Tunnel in West Virginia during the early 1870s (see Figure 2).[viii]

Figure 2. Operational Land Image (OLI) of the Big Bend Tunnel and its surrounding landscapes, including the Big Bend Mountain. Photograph by Wanmei Liang on August 23, 2024. NASA Earth Observatory. Public Domain
Set in a time of rapid industrialization, the story seethes sweat and steam. John Henry, with the use of a nine-pound hammer, pushes himself to beat a then emerging technology—the mechanical steam drill—in a steel-driving contest. He succeeds in the battle with the machine. Only mere seconds after winning, however, his heart stops, forever. In the late nineteenth century, John Henry’s tale, imbuing determination and hard work with caution, was popular among railroad and tunnel workers, becoming a more widely known story in the following decades.[ix] Since then, the story has taken multiple forms. As the Southern songs documented in Zora Neale Hurston’s momentous Mules and Men.[x] Also, as historical arguments about John Henry’s origins as an incarcerated labourer at the Virginia State Penitentiary, ultimately passing away from the silica dust exposure that was far too common in railroad and tunnel construction.[xi]
In 1978, a century after the folktale’s emergence, James met farmer John Henry Martin (1907-1989). Born on October 16, 1907, Martin grew up in North Carolina, within the sharecropping system built in the Reconstruction era. Upon purchasing a seventy-five acre farm, the pressures of peonage and indebted labour that had determined so much of Martin’s early life did not fade. In fact, they sharpened into painful relief as he worked to pay off the loan he used to obtain his farm. And, as his life progressed, he paid, more and more, in immeasurable sums as he began developing different chronic illnesses, including high blood pressure, severe stomach ulcers and arthritis. The latter pushed him to stop farming in the 1970s.[xii] In the same decade, the Big Bend Tunnel, largely built by Black American & Irish workers, closed due to compounding maintenance issues and rockfalls. Today, the site remains home to an unmarked burial ground for all the labourers whose lives ended while building the railway infrastructure, and to a statue of John Henry, yielding his historic hammer.[xiii]
When James coalesced Martin’s biography and the John Henry folktale into an explanatory model for cardiovascular health, he imagined John Henryism as an ambitious and hard-working personality type, a coping strategy for life under precarity.[xiv] But, when looking at the man, the myth and the model attached to both, I see far more than an internalized psychological profile. I see the Black feminist makings of what theorist Zakiyyah Iman Jackson calls “sub/super/humanization,” or what, before that, anthropologist Leith Mullings termed “Sojourner Syndrome.”[xv] I see how extractive economies mold circulatory systems from the outside in, just as they pressured the construction of the widespread Big Bend Tunnel. In some cases, they can arrest circulation entirely, pumping bodies to extreme limits and tragically halting livelihoods in their tracks.
Model 3
The final model I will describe here requires additional historical and spatial transitions. So, we move to a place that is the point of departure of my earliest memories, as well as my emerging ethnographic project: Montreal, Canada. To be precise, October 8th 1935 Montreal. On this date, Dr. Norman Bethune (1890-1939) pens a letter to a close friend, artist Marian Scott, asking her for advice about taking on a new position. A renown thoracic surgeon and persistent advocate for free, universal healthcare, the position he was contemplating was not a medical promotion, but to become the chair of the Friends of the Soviet Union Committee in Montreal.
In the letter, he expresses uncertainty and conviction at once:
Well, what shall I do? Do you think I can conscientiously take this job? I don’t think I know enough. I feel very ignorant. Yet I feel a tremendous impulse to do, to act. I hate to be thought one of the intelligentsia who talk and talk and talk and behind their words you feel their hearts are cold and it’s only an intellectual conundrum, a game.[xvi]
Sent from 1237 Rue Guy, only a 5 minute walk from where a commemorative statue of Bethune now stands in downtown Montreal, the letter contained not only words, but also a watercolour painting by Bethune himself (see Figure 3).
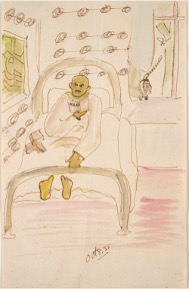
Figure 3. Norman Bethune Sick in Bed. 8 October 1935. Library and Archives Canada/Acc. No. 1995-115-193/010930935. In Marian Scott Collection. Public Domain.
At the time, Bethune was ill with jaundice, a condition stemming from a build up of bilirubin, a yellow pigment, and a hemolytic breakdown of red blood cells. Hemolysis is a rather opaque reaction where one’s own blood begins to destroy itself. The limpid watercolour depicts the doctor resting in bed as he reads Marx. While he ultimately turned down the position, by the end of 1936, he would find himself thrust across the Atlantic, in the middle of anti-fascist efforts during the Spanish Civil War.
Lasting less than a year, Bethune’s time in Spain could be broken down in hemolytic terms too, as it is known as a rather opaque and, in some accounts, self-destructive period of his life.[xvii] In a way, he maybe predicted this tumultuous time himself in the closing sentences of his letter to Scott, where he describes his own familial lineage in destructively fierce terms:
I come of a race of men, violent, unstable, of passionate convictions and wrongheadedness, intolerant yet with it all a vision of truth and a drive to carry them on to it even though it leads, as it has done in my family, to their own destruction—as it did my father.[xviii]
This short-lived moment has left a historically long-lasting trace. In support of the leftist Republican movement, Bethune would design the first mobile blood transfusion unit to transport blood to treat people injured in the frontlines of the war (see Figure 4).
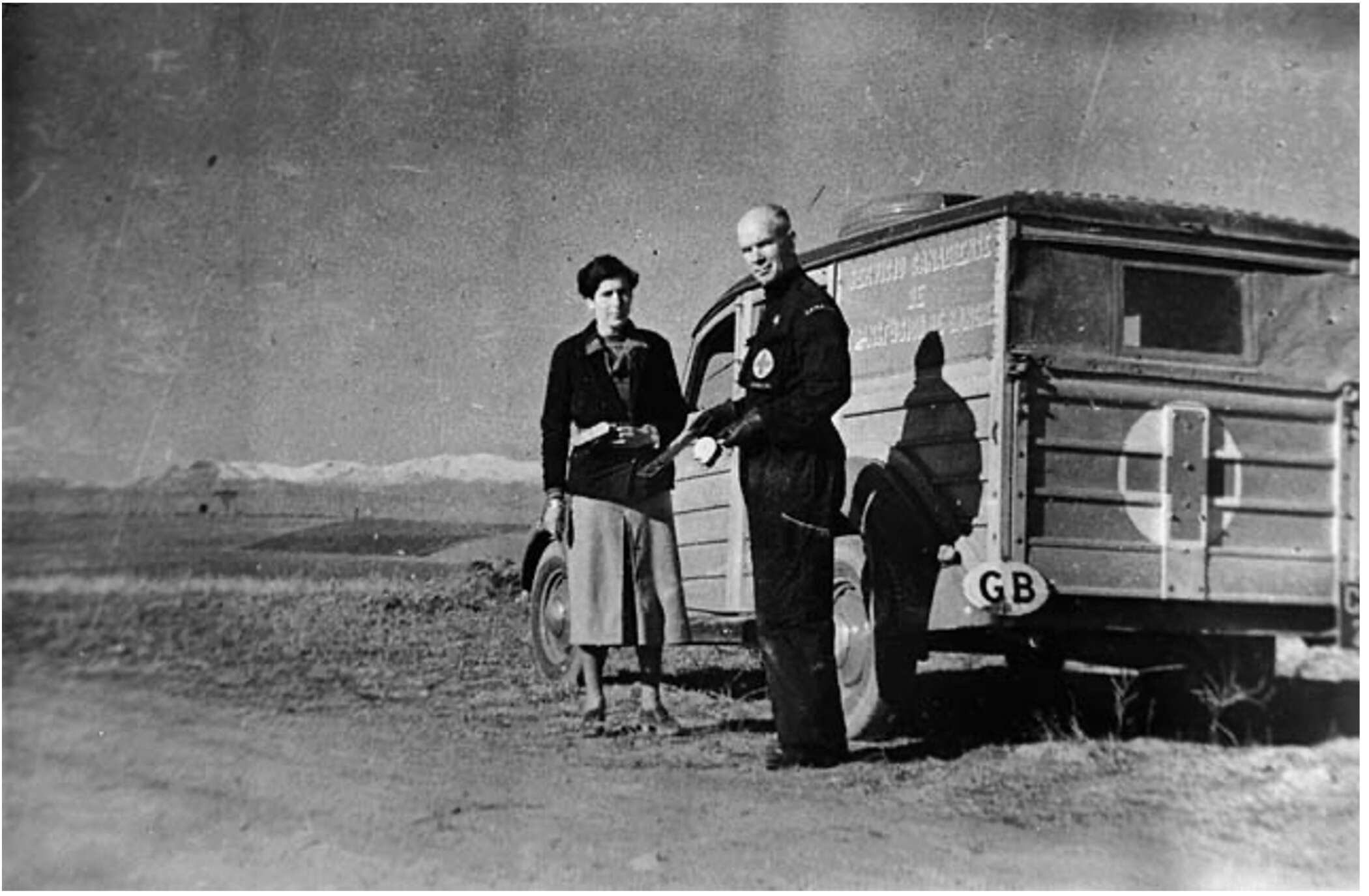
Figure 4. Canadian Blood Transfusion Unit which operated during the Spanish Civil War. Unknown photographer. Dr. Norman Bethune is at the right. Library and Archives Canada/PA-117423. In Hazen Edward Sise Collection. Public Domain.
Bethune died in 1939 from septicaemia, originally a cut on the finger, sustained while operating on the leg of a soldier. This final operation took place in China amidst the Second Sino-Japanese War, which he joined in further pursuit of an anti-imperialist world.[xix] The cataclysmic blood infection that led to Bethune’s death catapulted the doctor into historical eminence across the—at times disparate, at times converging—fields of biomedicine and internationalist political movements.[xx]
When we follow these kinds of trajectories, what becomes of blood, as well as the institutions and forms of knowledge that are tied to its representations? Conventional charts and schemas have been trusted guides in my early learning of blood circulation and transfusion science. Somehow, though, they always led me to more storied representations. To John Henry’s heavy hammer, resting in the fine dust that sweeps across the abandoned lives and railways that built the paths of this nation’s circulation. To the sickles and sicknesses of historical struggles that brought me to retrace global histories in the corners of streets I have walked through countless times. To the sanguine radioactivity of Reference Man, literally squaring the tragedy of our nuclear surround. All these cases have taught me the same thing: that the best models are not necessarily those that succeed in emulating every body, but those that push us to adjust how and where we perceive bodies in the first place.
Endnotes
[i] Eckerman & Cristy, “The Reference Individual of Radiation Protection.” Workshop presentation.
[ii] Cristy, Reference Man Anatomical Model, 4.
[iii] Leggett, Williams & Eckerman, A Blood Circulation Model for Reference Man, 4.
[iv] Cram, Unmaking the Bomb, 35. For example, Cram elucidates how the Reference Man/Person is not always calibrated to account for higher radiogenic risks that women and children face.
[v] To view the original model from Figure 1, see Leggett, Williams & Eckerman, A Blood Circulation Model for Reference Man, 4.
[vi] James et al. “John Henryism and Blood Differences Among Black Men.” See also James et al. “Socioeconomic Status, John Henryism and Hypertension in Blacks and Whites.” American Journal of Epidemiology. See also James et al. “Socioeconomic Status, John Henryism, and Blood Pressure in Black Adults: The Pitt County Study.”
[vii] “Conquering the Quiet Killer,” TIME Magazine, January 13, 1975.
[viii] James, “John Henryism and the Health of African-Americans,” 166; 179. To view Figure 2, see Voiland, “Laboring at the Big Bend Tunnel,” NASA, September 2, 2024.
[ix] Ibid. See also James, “The Narrative of John Henry Martin,” Southern Cultures, Inaugural Issue (1993): 84.
[x] See Hurston, I Love Myself When I Am Laughing… And Then Again When I Am Looking Mean and Impressive: A Zora Neale Hurston Reader.
[xi] Nelson, Steel Drivin’ Man: John Henry, the Untold Story of an American Legend, 89.
[xii] James, “The Narrative of John Henry Martin,” 103–104.
[xiii] National Park Service, “John Henry and the Coming of the Railroad.”
[xiv] Colburn, “Cover Story – All in a Day’s Work: It Can Add Meaning or Misery to Life,” Washington Post, January 29, 1986. For a more recent application, see also Jamison, “The Pain of Perfectionism,” The New Yorker, August 4, 2025.
[xv] Jackson, Becoming Human, 48. To see how Mullings described Sojourner Syndrome in relation to John Henryism, see also Mullings, “Resistance and Resilience: The Sojourner Syndrome and the Social Context of Reproduction in Central Harlem, 86.
[xvi] Hannant (eds.), Norman Bethune’s Writing and Art, 82.
[xvii] Hannant, Norman Bethune’s Writing and Art, 118.
[xviii] Hannant, Norman Bethune’s Writing and Art, 82.
[xix] Hannant, Norman Bethune’s Writing and Art, 358–359.
[xx] For an example of the kinds of convergences between medicine, anthropology and radical politics that Bethune inspired, by way of the work of the late anthropologist and physician Sam Dubal, see Jason P. Price, “Introduction: An Invitation to Rebel Kinship,” Society of Medical Anthropology, 2024. See also Dubal, Samrab & Janeway, “Beyond border health: Infrastructural violence and the health of border abolition.”
This post was curated by Contributing Editor Tiên Dung Hà, and reviewed by Contributing Editor Jackie Ashkin.
References
Colburn, D. (1986, January 29). “Cover Story – All in a Day’s Work: It Can Add Meaning or Misery to Life.” Washington Post.
(1975, January 13). “Cover Story – Conquering the Quiet Killer.” TIME Magazine.
Cram, S. (2023). Unmaking the Bomb: Environmental Cleanup and The Politics of Impossibility. Oakland: University of California Press.
Cristy, M. (1994). Reference Man Anatomical Model. Oak Ridge: Oak Ridge National Laboratory.
Dubal, S., Samrab, S. S. , & Janeway, H. H. (2021). “Beyond border health: Infrastructural violence and the health of border abolition,” Social Science & Medicine 279: 1–8.
Eckerman, K.F., & Cristy, M. (1995). The Reference Individual of Radiation Protection. Oak Ridge: Oak Ridge National Laboratory. Presented at workshop on voxel phantoms in Chilton, United Kingdom, July 1995.
James, S. A. (1994). “John Henryism and the Health of African-Americans.” Culture, Medicine & Psychiatry 18: 163–182.
James, S. A. (1993). “The Narrative of John Henry Martin.” Southern Cultures (Inaugural Issue): 83–106.
James, S. A., Hartnett, S. A, & Kalsbeek, W. D. (1983). “John Henryism and Blood Pressure Differences Among Black Men.” Journal of Behavioral Medicine 6(3): 259–278.
James, S.A., Keenan, N. L., Strogatz, D. S., Browning, S. R., & Garrett, J. M. (1992). “Socioeconomic Status, John Henryism, and Blood Pressure in Black Adults: The Pitt County Study.” American Journal of Epidemiology 135: 59–67.
James, S.A., Strogatz, D. S.,Wing, S.B., & Ramsey, D. (1987). “Socioeconomic Status, John Henryism and Hypertension in Blacks and Whites.” American Journal of Epidemiology 126: 664–673.
Jamison, L. (2025, August 4). “The Pain of Perfectionism.” The New Yorker.
Hannant, L. (eds). (1996). Norman Bethune’s Writing and Art. Toronto: University of Toronto Press.
Hurston, Z. N., & Walker, A. (2020). I Love Myself When I Am Laughing… And Then Again When I Am Looking Mean and Impressive: A Zora Neale Hurston Reader. New York: The Feminist Press at CUNY.
Jackson, Z. I. (2020). Becoming Human: Matter and Meaning in an Antiblack World. New York: NYU Press.
Leggett, R. W., Williams, L. R., & Eckerman, K.F. (1996). A Blood Circulation Model for Reference Man. Oak Ridge: Oak Ridge National Laboratory.
Mullings, L. (2005). “Resistance and Resilience: The Sojourner Syndrome and the Social Context of Reproduction in Central Harlem.” Transforming Anthropology 13(2): 79–91.
National Park Service. (2023, September 14). “John Henry and the Coming of the Railroad.” New River George: National Park & Preserve West Virginia.
Nelson, S. R. (2006). Steel Drivin’ Man: John Henry, the Untold Story of an American Legend. Oxford: Oxford University Press.
Voiland, A. (2024, September 2). “Laboring at Big Bend Tunnel.” National Aeronautics and Space Administration.

.jpg){kind=link}