This special series examines the spatial, temporal, and conceptual boundaries of infection. As a primarily analytic approach, the authors in this series unpack epidemiologic keywords such as outbreak, hotspot and epidemic, to assess their uptake, uses and meanings amongst scientists, public health and healthcare practitioners, experts and broader publics. As disruptions to public health ripple through the healthcare landscape in the United States[1], and whilst the global COVID-19 pandemic continues to haunt our collective present, the fundamental terms or “keywords” through which we understand disease transmission demand ethnographically-grounded inquiry, critique, and theorization. The posts in this series look at how infectious diseases and their conceptualizations spread through space and time, as well as how ethnography can articulate the expansive, lived realities of infection.
By (un)grounding keywords in the work of disease modeling and through the experiences of those caring for and living with infectious disease, this series seeks to uproot such epidemiological concepts from the grip of biomedicine and its claims to defining and characterizing what infection is (Briggs 2024). Specifically, we ask, how can medical anthropologists and science and technology studies scholars expand these keywords in ways that are analytically useful to transdisciplinary understandings of infectious disease? How can “anthropology-with-two-feet-on-the-ground” (Scheper-Hughes 1993) revise or speak back to these keywords, thus troubling the boundaries that they reproduce and reify? How do keywords condense long-term social and economic conditions into public health “crises,” and what are some frameworks and vernaculars for experiencing, detecting, and defining infectious disease otherwise?
Why Space? Why Temporality?
Imagining the spaces through which infection spreads has been central to how disease is known and populations are governed. British physician John Snow’s canonical “dot-map” of cholera cases clustered around the Broad Street water pump in nineteenth-century London exemplifies how disease has long been rendered legible through spatial visualization, proximity, and enclosure (Johnson 2006; Trostle 2005). Snow’s map did more than identify a source of contagion. It produced a particular spatial ontology of disease, one in which infection could be localized, bounded, and intervened upon through the reorganization of urban infrastructure. The management of disease spread and surveillance of bodies in space has been central to the entrenchment of biopower, which is the control of human populations through interventions on their health and other biological parameters. Biopower as a dominant form of liberal governance emerged in Europe during the nineteenth century, particularly in relation to cholera epidemics (Foucault 2008; Cohen 2009). Social scientific and humanistic scholarship has since denaturalized such spatial logics by emphasizing that space is neither neutral nor pre-given but always relational, socially produced, and deeply entangled with histories of race, gender, and power (Lefebvre 1991; Massey 2005; Shabazz 2015).
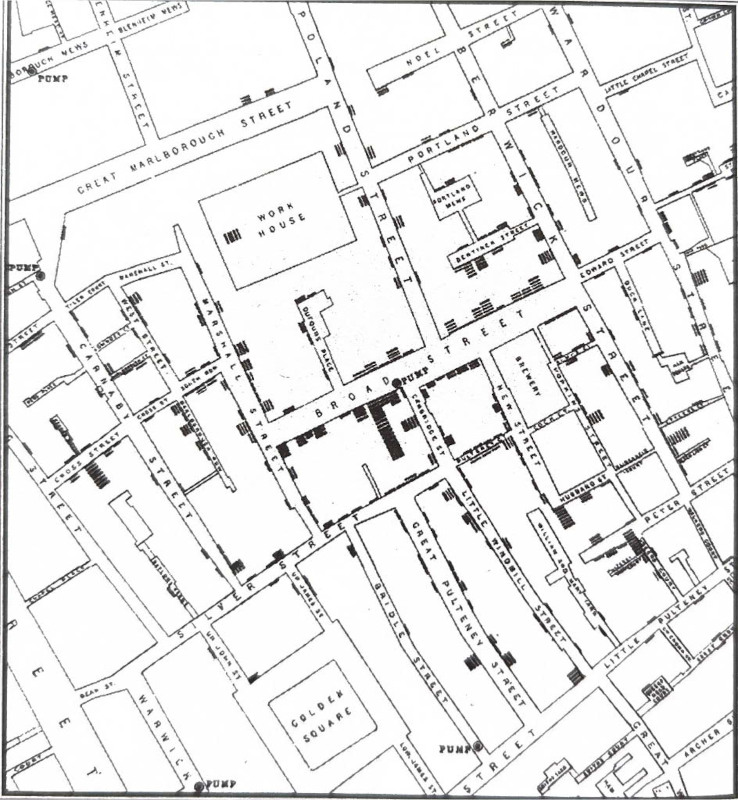
John Snow’s cholera dot map near the Broad Street water pump was one of the first use of spatial visualization in epidemiology. This photograph was taken from Johnson, Steven’s “The Ghost Map: The Story of London’s Most Terrifying Epidemic – and How It Changed Science, Cities, and the Modern World,” published in 2007 by Riverhead Books (page 190). Credits: Katharina Rynkiewich.
Imagining spaces of infection also entails the demarcation of spaces where infection has not yet arrived. A space without infection does not necessarily remain free of disease, but rather can be vulnerable to the movement of bacteria or viruses across established boundaries. Mary Douglas’s (1966) term “matter out of place” is instructive in cases of such contamination, as it signals how microbes broach social, spatial, and temporal boundaries and, in doing so, elicit a response. For example, Teresa MacPhail (2014) has written about the global enterprise of pandemic preparedness that continually, and often ineffectually, works to monitor and control the movements of pathogenic matter (such as SARS, H1N1, etc.) within and across boundaries. Even in lieu of disease transmission, fears of disease outbreak can also spread and contaminate the spaces and structures that humans inhabit, what Carlo Caduff (2015) describes as “plague visions.”
Public health institutions often model infection as an acute, exceptional, unexpected crisis, elaborating a “state of exception” (Agamben 1999) under which the amplification of strategies and techniques to surveil and contain the movement of bodies becomes rationalized and normalized (Foucault 2008) These exceptional measures can also extend beyond the temporal limits of public health crisis to structure intermediary periods between publicly-recognized disease outbreaks. The defining point of an epidemic begins by distinguishing a moment of rupture in which a disease begins to spread between persons more rapidly within a given place across a period of time (Trostle 2005; Cerón 2018, 105). These models of disease temporalize infection into a linear chronology that spans across phases of preparedness (or lack thereof), outbreak, peak, and resolution. Timelines around the spread of infectious disease are multiple and subject to contestation, mired in questions of who decides when outbreaks end and for whom. For example, the Biden administration’s declared “end” of the COVID-19 pandemic in spring 2023, even when many groups remained vulnerable to infection, put an end to programs for socioeconomic support and expanded healthcare access that had emerged during the period when it was still seen as a public health emergency (Death Panel 2021).
The hypervisibility and acuity of public health crisis overshadows the “slow violence” of the cumulative, transgenerational effects of land dispossession, labor exploitation, and structural barriers to healthcare. Rather than possessing the visibility, immediacy, and acuity that characterize events of spectacular violence, slow violence is gradual, seemingly imperceptible, and “disperse[s] across time and space” (Nixon 2011, 2). It materializes through chronic, non-communicable diseases such as metabolic illness, cancers, immunological disorders (Yates-Doerr 2015; Moran-Thomas 2019). The distinction between infectious, communicable diseases and non-infectious, noncommunicable diseases obscures the persistence of structural conditions that make certain populations more vulnerable to illness and “slow death” (Berlant 2007). Historically, the production of crisis has served to stabilize and normalize particular institutions and conditions that perpetuate structural and systemic harms (Masco 2017). A critical engagement with the spatial and temporal dimensions of infection guide our effort to interrogate how infectious disease is bounded, narrated, and acted upon, and how alternative ways of apprehending space and time might reconfigure what and who counts in an outbreak.
Why Keywords? Why Ethnography?
We have organized this special issue according to keywords that circulate in global public health discourse, particularly in the documenting, reporting, and epidemiological modeling of infectious diseases. As scholars of critical medical anthropology and public health studies, our work has examined how infectious diseases are shaped and understood through diverse, situated practices (Lu 2024; Rynkiewich 2021, 2023; Imbert, Kinley, et al. 2021). As ethnographers working in collaboration with public health practitioners and policymakers, we have become attuned to the social lives that keywords in epidemiological modeling take on in and beyond settings of disease prevention, monitoring, and care. Keywords have a certain boundedness, demarcating conceptual spaces (Williams 2014). Yet, they are also subject to multiple interpretations, inviting more capacious understandings of such conceptual spaces. Inspired by a variety of similar projects in the critical social sciences and humanities (see also, Altschuler, Metzl, and Wald 2023; Howe and Pandian 2019), we have invited contributors to think with keywords as a starting point for analysis. Some are productively juxtaposed, while others form the basis for critique or provide a starting point for generating new concepts. Ethnographically (un)grounding epidemiological keywords is a way of problematizing the ways in which forms of health and medical knowledge, populations, and infection itself are bounded or unbounded across space and time.
A critical engagement with studies of infectious diseases involves dismantling and reconstructing terminologies of disease spread in order to identify their underlying assumptions and associated effects. It entails tracing how keywords are de- and re-contextualized between and amongst public health workers, patients, care providers, and broader publics in an effort to expand, connect, and multiply their meanings and uses. Such keywords illuminate how different imaginaries of “public” and “health” bring about diverse practices, discourses, and materialities of our collective movements, proximities, and ways of co-habiting places. Strategies of viral management for COVID-19, for example, restricted movements and ordered bodies in space through measures such as social distancing, sheltering in place, masking, and sanitation practices. Images and slogans such as “flattening the curve” and “stop the spread” abounded early on, simultaneously translating epidemiological concepts to publics and applying them to immediate public health praxis.
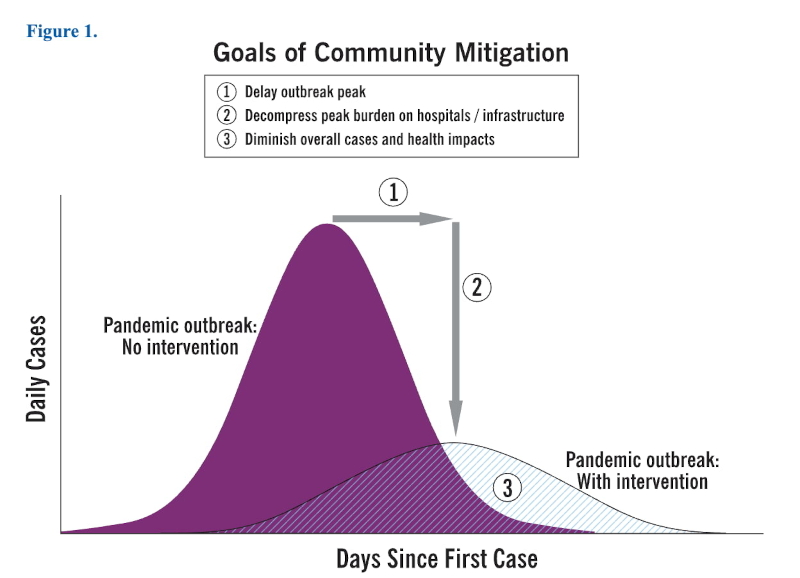
Chart depicting effects of disease prevention measures in lowering an acute spike in caseload, thus flattening the curve. Credits: Centers for Disease Control and Prevention (U.S.) “Interim pre-pandemic planning guidance : community strategy for pandemic influenza mitigation in the United States: early, targeted, layered use of nonpharmaceutical interventions” (2007). Accessed here: https://stacks.cdc.gov/view/cdc/11425.
The ungovernability of life, along with ensuing efforts and strategies to make life governable, have been foundational to state formation and legitimacy (Dewachi 2017). Technoscientific surveillance and the demarcation of boundaries at particular and critical moments in time serve to alleviate the disease-causing effects of infection (MacPhail 2014). Imperial and national governance has long drawn on the logics of sanitation and hygiene to justify the exclusion and racialization of groups of people (Stern 1999; Zulawski 2000; Wilson 2004; Molina 2010; Bivins 2015). However, as witnessed during early stages of the emerging COVID-19 pandemic, public health safety measures did not seem to apply when it came to incarcerated persons (Tosh et al. 2020) and migrant laborers (Garcia-Colón 2020). In other contexts, such as homeless shelters, local public health officials simply could not implement many of these safety measures due to crowded conditions and other constraints (Imbert et al. 2020). Furthermore, the models of communicability that medical authorities have used to describe infection have historically excluded and delegitimized other forms of medical and health knowledge about how and why illness spreads (Briggs & Mantini-Briggs 2016; Farmer 2006).

CDC poster depicting precautions to mitigate respiratory disease transmission. Credits: National Center for Immunization and Respiratory Diseases (U.S.). Division of Viral Diseases. “Coronavirus Disease 2019 (COVID-19): Stop the spread of germs: 2/6/2020” (2020). Accessed here: https://stacks.cdc.gov/view/cdc/84899/cdc_84899_DS1.pdf
The contributors in this series draw from distinct historical moments and ethnographic settings to follow the social lives of epidemiological keywords. Alejandro Cerón examines how decisions around epidemic “mitigation” navigate a tense interplay between technical expertise and political imperative, tracing how the modern myth of John Snow has shaped public health professional identity and epidemiological authority. Katharina Rynkiewich draws from research in South Florida, USA, to show a need for expanding the concept of “hotspots” to encompass uncentered and intermittent spaces of infection. Joyce Lu examines how the concept of disease “carrier” becomes attached to persons, animals, and other mobile things as well as incorporated into bodily habitus in highland Guatemala. Pat Kinley draws on their experience conducting contact tracing for two “index cases” of COVID-19 in a San Francisco homeless shelter to demonstrate how slow violences of gentrification, displacement, and neglect materialize through interrelated processes of space compression and disease vulnerability. Alex (Chuan Hao) Chen examines the keyword “leak” from the perspective of laboratory architecture, exploring how the material and architectural conceptions of laboratories provide fertile ground for rumors and suspicion.
The epidemiologic and public health vocabularies employed to characterize and intervene upon the spread of infection demarcate the spatial and temporal boundaries of where infection is expected to be, where it is anticipated to travel, and how experts and communities might mitigate its spread. The double bind (Bateson et al. 1956; Fortun 2001, 13, as cited in Callison 2014) of communicating information about infectious disease spread is that it requires trust in the methods, technologies, and institutions that produce and negotiate them. Yet at the same time, models, policies, and discourse on infection must be transported into the popular imagination in ways that meaningfully shape collective values, actions, and futures. (Un)grounding keywords through ethnography also provides us with the opportunity to productively incorporate while systematically critiquing historically used terminologies of marginalization and racialized structural violence. Taking stock of and reconceptualizing currently used keywords promises to broaden horizons of collective health and wellbeing.
We invite further additions to this series. Interested contributors should reach out to Joyce Lu (jl2295@rwjms.rutgers.edu) by July 1, 2026, with a short abstract (100-200 words).
Footnote
[1] In the year 2025, agencies like the National Institute of Health and the National Science Foundation have had budget cuts, department closings, and a scale back approach that has led to depictions of a decimated public health funding landscape in the United States. Also see Cutler and Glaeser 2025 for more details.
Acknowledgement
This post was curated by Contributing Editor Tayeba Batool, reviewed by Contributing Editor Melina Campos, and translated into Spanish by Contributing Editor Karina Aranda.
References
Agamben, Giorgio. 1998. Homo Sacer: Sovereign Power and Bare Life. Stanford University Press.
Altschuler, Sari, Jonathan Metzl, and Priscilla Wald, eds. 2023. Keywords for the Health Humanities. NYU Press.
Bateson, Gregory, Don D. Jackson, Jay Haley, and John Weakland. 1956. “Toward a Theory of Schizophrenia.” Behavioral Science 1 (4): 251–264.
Berlant, Lauren. 2007. “Slow Death (Sovereignty, Obesity, Lateral Agency).” Critical Inquiry 33 (4): 754-780.
Bivins, Roberta. 2015. Contagious Communities: Medicine, Migration, and the NHS in Post War Britain. First edition. University Press.
Briggs, Charles, and Clara Mantini-Briggs. 2016. Tell Me Why My Children Died: Rabies, Indigenous Knowledge, Communicative Justice. Duke University Press.
Briggs, Charles L. 2024. Incommunicable: Toward Communicative Justice in Health and Medicine. 1st ed. Duke University Press.
Caduff, Carlo. Pandemic Perhaps: Dramatic Events in a Public Culture of Danger. 2015. University of California Press.
Callison, Candis. 2014. How Climate Change Comes to Matter: The Communal Life of Facts. Experimental Futures. Duke University Press.
Cerón, Alejandro. 2018. Epidemiología neocolonial: prácticas de salud pública y derecho a la salud en Guatemala. Avancso.
Cohen, Ed. 2009. A Body Worth Defending: Immunity, Biopolitics, and the Apotheosis of the Modern Body. Duke University Press.
Dewachi, Omar. 2017. Ungovernable Life: Mandatory Medicine and Statecraft in Iraq. Stanford University Press.
Douglas, Mary. 1966. Purity and Danger: An Analysis of Concepts of Pollution and Taboo. Routledge.
Farmer, Paul. 2006. AIDS and Accusation: Haiti and the Geography of Blame. University of California Press.
Foucault, Michel. 2008. The Birth of Biopolitics: Lectures at the Collège de France, 1978-79. With Michel Senellart and Collège de France. Palgrave Macmillan.
García-Colón, Ismael. 2020. “The COVID-19 Spring and the Expendability of Guestworkers.” Dialectical Anthropology44 (3): 257–64.
Imbert, Elizabeth, Patrick M. Kinley, Ashley Scarborough, Caroline Cawley, Madeline Sankaran, Sarah N. Cox, Margot Kushel, Juliet Stoltey, Stephanie Cohen, and Jonathan D. Fuchs. 2021. “Coronavirus disease 2019 outbreak in a San Francisco homeless shelter.” Clinical Infectious Diseases 73 (2): 324-327.
Johnson, Steven. 2007. The Ghost Map: The Story of London’s Most Terrifying Epidemic–and How It Changed Science, Cities, and the Modern World. Riverhead Books.
Lefebvre, Henri. 1991. The production of space. Blackwell.
Lu, Joyce. 2024. “Microbial Semiotics: Sites of Ideological Work in Antibiotic Resistance.” American Anthropologist 126 (4): 694–98. https://doi.org/10.1111/aman.28006.
MacPhail, Theresa. 2014. The Viral Network: A Pathography of the H1N1 Influenza Pandemic. Cornell University Press.
Masco, Joseph. 2017. “The Crisis in Crisis.” Current Anthropology 58 (S15): S65–76. https://doi.org/10.1086/688695.
Massey, Doreen. 2005. For Space. Sage.
McKay, Richard. 2017. Patient Zero and the Making of the AIDS Epidemic. University of Chicago Press.
Molina, Natalia. 2010. “‘In a Race All Their Own’: The Quest to Make Mexicans Ineligible for U.S. Citizenship.” Pacific Historical Review 79 (2): 167–201. https://doi.org/10.1525/phr.2010.79.2.167.
Moran-Thomas, Amy. 2019. “What Is Communicable? Unaccounted Injuries and ‘Catching’ Diabetes in an Illegible Epidemic.” Cultural Anthropology 34 (4): 4. https://doi.org/10.14506/ca34.4.01.
Pandian, Anand and Cymene Howe, eds. 2020. Anthropocene Unseen: A Lexicon. Punctum Books.
Rocco, Phil, Beatrice Adler-Bolton, and Artie Vierkant. 2021. “The Sociological Production of the End of the Pandemic.” Death Panel. February 4, 2021. https://www.deathpanel.net/transcripts/the-sociological-production-of-the-end-of-the-pandemic-covid
Rynkiewich, Katharina. 2021. “Everyday Infection, Looming Threat: Hospital-Based Infection Control in the United States.” Somatosphere. February 9, 2021. https://somatosphere.com/2021/hospital-infection-control-medical-anthropology.html/
Rynkiewich, Katharina, Sarin Gole, Sarah Won, David N Schwartz. 2023. “Cultures of antibiotic prescribing in medical intensive care.” Social Science & Medicine 324: 1-7. https://doi.org/10.1016/j.socscimed.2023.115834
Scheper-Hughes, Nancy. 1993. Death Without Weeping: The Violence of Everyday Life in Brazil. University of California Press.
Shabazz, Rashad. 2015. Spatializing Blackness: Architectures of Confinement and Black Masculinity in Chicago. University of Illinois Press.
Stern, Alexandra Minna. 1999. “Buildings, Boundaries, and Blood: Medicalization and Nation-Building on the U.S.-Mexico Border, 1910-1930.” Hispanic American Historical Review 79 (1): 41–81. https://doi.org/10.1215/00182168-79.1.41.
Tosh, Sarah R., Ulla D. Berg, and Kenneth Sebastian León. 2021. “Migrant Detention and COVID-19: Pandemic Responses in Four New Jersey Detention Centers.” Journal on Migration and Human Security 9 (1): 44–62. https://doi.org/10.1177/23315024211003855.
Trostle, James A. 2005. Epidemiology and Culture. Cambridge University Press.
United States Centers for Disease Control (CDC). n.d. “Stop the Spread of Germs (COVID-19).” U.S. Department of War. Accessed January 16, 2026. https://www.war.gov/Multimedia/Photos/
