What do you call a practice that is neither traditional nor modern, neither fully inside medicine nor fully outside it? In Türkiye, the answer arrived in the form of an acronym: GETAT (Geleneksel ve Tamamlayıcı Tıp) or Traditional and Complementary Medicine. Officially regulated since 2014, it now encompasses everything from acupuncture and cupping to phytotherapy and leech therapy, all performed legally only by licensed physicians in certified facilities. On paper, it sounds like a tidy administrative solution. In the field, it turned out to be anything but.[1] We began to understand this early, in a clinic in Ankara, when one of the physicians who had helped draft the original regulations leaned back in his chair and said: “GETAT is the best name.” The term, he explained, had not emerged locally, but was shaped through years of visits to countries known for their traditional medicine systems: China, India, Thailand, Germany. “We looked at how they classify it,” he continued. “What counts as traditional? What counts as complementary, holistic or integrative? You cannot just translate these things. You have to adapt them.” The controversy over the label itself signaled historical and sociological divisions around medical knowledge and expertise.
Over the past decade, traditional, complementary, and alternative medicine has moved from the margins of healthcare systems into their institutional core. In Türkiye, this transformation has taken a particularly visible form through the increasing institutionalization of Traditional and Complementary Medicine at state hospitals via GETAT. Yet, as this encounter suggests, GETAT is not merely the institutional recognition of pre-existing practices. It is the outcome of a series of translations, adaptations, and negotiations that reshape what counts as medicine in the first place. In this sense, it can be understood as a hybrid entity (Latour 1993): a formation that does not belong neatly to either “modern” biomedicine or “traditional” healing, but instead emerges through the entanglement of heterogeneous elements including scientific protocols, cultural practices, regulatory frameworks, and global circulations of knowledge.
It was this hybridity that puzzled us as we made our way into the field. For example, when we entered a private hospital in Ankara that advertised its “natural” treatments, what immediately caught our attention were large promotional posters in the waiting area: GETAT practices and medical aesthetic procedures were displayed side by side, equally prominent, equally marketable. Rather than occupying separate domains, healing and beautification appeared as part of the same continuum.

Side-by-side advertisements in a private hospital in Ankara: a medically supervised weight-loss and aesthetic program alongside “traditional treatments,” illustrating the convergence of biomedical, aesthetic, and traditional approaches to bodily care. Image by the author.
In conversation with one of the physicians this alignment became even more explicit. He spoke at length about feeling significantly younger not just thanks to practices such as phytotherapy and acupuncture, but also due to Botox treatments and a healthy lifestyle. In this setting, GETAT was no longer only about treating illness. It was part of a broader project of caring for and optimizing the self—what Nikolas Rose (1999), building on Foucauldian notions of self-governance, describes as the governing of the self. Health and beauty, treatment and maintenance, discipline and consumption were not separate concerns, but deeply intertwined practices.
From Dissatisfaction to Reconfiguration
The growing interest in traditional and complementary medicine is often explained through dissatisfaction with biomedicine. Biomedical approaches, grounded in a Cartesian separation of mind and body, have long been criticized for reducing the body to a mechanistic object, detached from social, psychological, and experiential dimensions. As Scheper-Hughes and Lock (1987) argue, bodies are always simultaneously biological, social, and lived. In Türkiye, this critique resonates strongly. Individuals increasingly turn to healing practices that promise a more “holistic” engagement with the body, practices that are culturally familiar and experientially meaningful. This shift is also reflected in how practitioners themselves describe a transformation in their clinical reasoning. One physician we spoke to contrasted their earlier biomedical training with their current approach:
“If someone had a headache, I would just prescribe a painkiller and send them off. That was all I knew. But now I ask: why does this person have a headache? Is it stress? Sleep? Diet? Anxiety? Something environmental? Before, my goal was just to stop the pain. But that doesn’t mean it won’t come back.”
For her, GETAT did not simply add new treatment options; it reoriented the very logic of care—from symptom management toward a more expansive inquiry into the conditions of life that produce illness. However, the rise of GETAT in Türkiye cannot be reduced to patient dissatisfaction alone. As the clinical encounter above suggests, what is shifting is not only where patients seek care, but how care itself is imagined and practiced. This transformation is also shaped by global governance regimes and institutional reconfigurations through which traditional healing, once situated outside formal medicine, is now brought into regulatory frameworks, standardized, and disciplined.
Optimizing Life
What is at stake in this alignment is not simply the coexistence of different medical traditions, but a subtle shift in how life itself is understood and acted upon. In the clinic, this shift was not articulated through abstract concepts, but through everyday practices and routines. Treatments such as cupping (hacamat), phytotherapy, or acupuncture were rarely presented as last-resort interventions. Instead, they were framed as ways of maintaining balance, preventing illness, and investing in one’s well-being over time. Posters, packages, and promotional campaigns reinforced this message, inviting patients to take an active role in managing their own health.
This orientation resonates with what Katherine E. Kenny (2015) describes as the economization of life, a mode of thinking in which life is treated as something that can be improved, extended, and optimized through ongoing investment. In this sense, health becomes less a state to be restored and more a project to be managed. At the same time, as Nikolas Rose and Ayo Wahlberg (2015) suggest, this involves a broader governmentalization of living, where individuals are increasingly called upon to monitor, regulate, and optimize their own bodies. The responsibility for health does not disappear from institutions, but it is redistributed—settling into everyday habits, routines, and choices of individuals.
In the Turkish context, GETAT becomes one of the sites where this redistribution takes place. Even practices grounded in religious traditions are reconfigured within this logic. The circulation of hijama calendars, for instance, which designate auspicious days for treatment according to lunar cycles, introduces a temporal discipline that aligns bodily care with rhythms of anticipation, planning, and optimization. Here, spiritual temporality and contemporary health practices do not stand in opposition. Instead, they become part of the same mode of care—one in which the body is continuously attended to, adjusted, and improved over time.
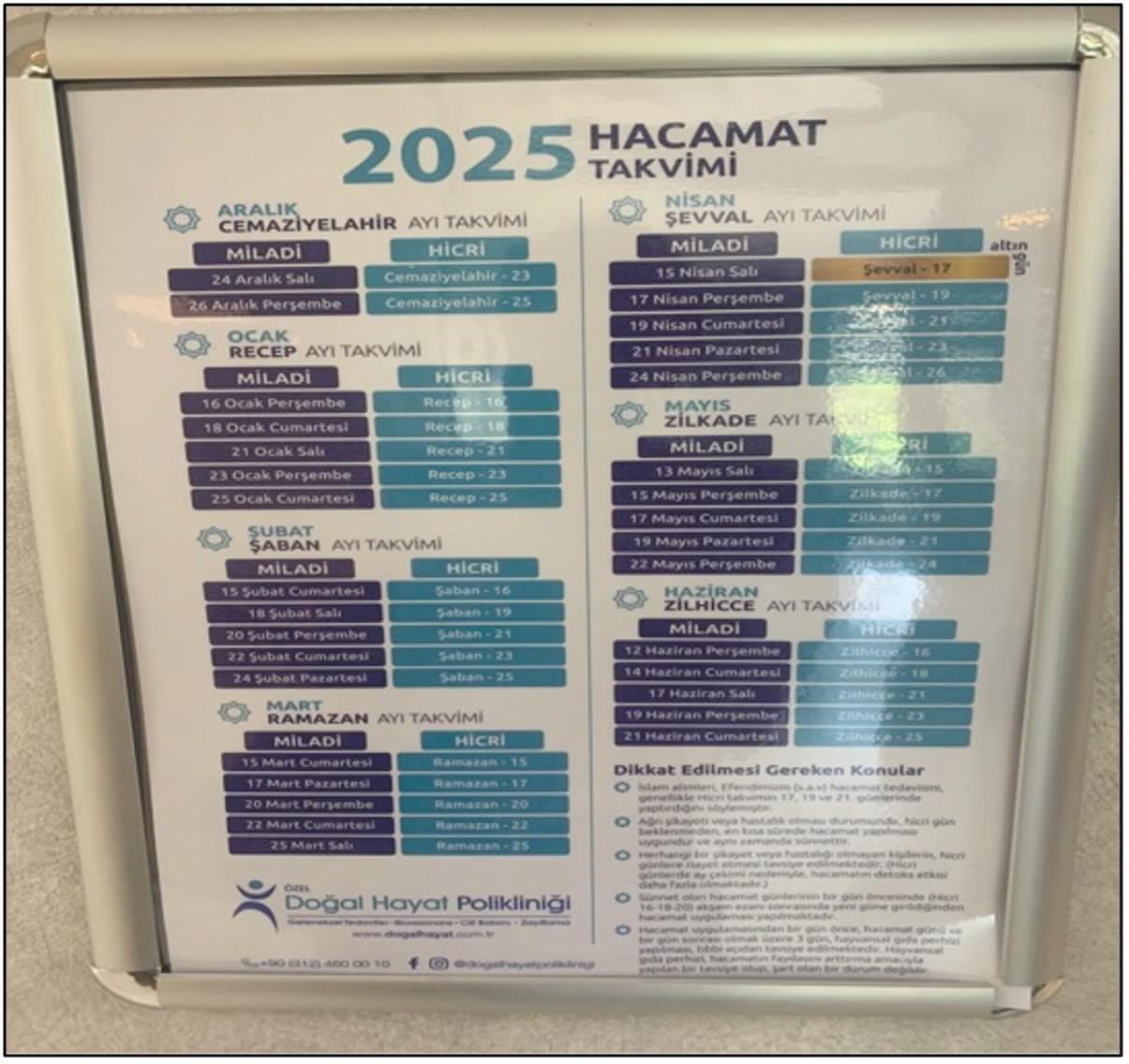
A 2025 hijama calendar in a private clinic, structuring treatment timing through lunar cycles. Image by the author.
Seen from this angle, the proximity between GETAT and aesthetic medicine is not incidental, but revealing. In many clinical settings, practices associated with healing appear alongside those associated with enhancement, blurring the line between treating illness and improving the body. Care, in this sense, becomes increasingly inseparable from consumption. Health is no longer defined solely as the absence of illness; rather, care becomes an ongoing project—one that requires constant attention and intervention.
At the same time, this expanding terrain of care raises persistent questions about legitimacy. What counts as “scientific” medicine? Which practices can be authorized, and which must remain outside? In Türkiye, these questions are not settled once and for all, but are continuously negotiated. Terms such as “complementary,” “integrative,” and “evidence-based” are mobilized in shifting ways, allowing certain practices to be incorporated into biomedical frameworks while excluding others.
For instance, phytotherapy is often translated into the language of laboratory research and clinical trials, while cupping is rendered acceptable when performed under sterile conditions by licensed physicians. In contrast, shrine-based or spiritually mediated practices remain outside the boundaries of legitimate medicine. The line between science and non-science is not dissolved, but actively redrawn in practice, reflecting what Gil Eyal (2019) describes as the ongoing negotiation of expertise and its boundaries.
What emerges, then, is not a simple coexistence of different medical systems, but a carefully managed form of hybridity. Traditional practices are selectively incorporated, standardized, and reassembled in ways that align with biomedical norms, while elements that resist such translation are marginalized or excluded. Ambiguity itself becomes a governing tool—allowing flexibility and adaptation, while maintaining control over what counts as valid knowledge.
Taken together, these dynamics suggest that the rise of GETAT in Türkiye is not simply a story of rediscovering tradition or resisting biomedicine. Rather, it reflects a broader transformation in how medicine, knowledge, and the body are being reconfigured. Individuals are increasingly positioned as responsible for managing their own health, not only as a matter of care, but as an ongoing project of optimization. GETAT sits at the intersection of these processes—not outside biomedicine, nor fully within it, but as a hybrid site where the boundaries of medicine are continuously made and remade.
[1] This blog post draws on ethnographic fieldwork conducted as part of an ongoing research project on Traditional and Complementary Medicine (GETAT) and medical knowledge production in Türkiye, including current work on Anatolian Medicine.
This post was curated by Contributing Editor Bronte Jones and reviewed by Andra Sonia Petrutiu.
References
Eyal, G. (2019). The crisis of expertise. Cambridge: Polity Press.
Kenny, K. E. (2015). The biopolitics of global health: Life and death in neoliberal time. Journal of Sociology, 51(1), 9–27.
Latour, B. (1993). We have never been modern. Cambridge, MA: Harvard University Press.
Rose, N. (1999). Governing the soul: The shaping of the private self (2nd ed.). London: Free Association Books.
Rose, N., & Wahlberg, A. (2015). Governing the molecular: Life science and the politics of health. Economy and Society, 44(1), 1–22.
Scheper-Hughes, N., & Lock, M. M. (1987). The mindful body: A prolegomenon to future work in medical anthropology. Medical Anthropology Quarterly, 1(1), 6–41.
